
Editor's note: The illicit drug trade is undergoing a seismic shift, with Utah in the middle of the deadly impact of opioids. This is the fourth story in an ongoing series about this modern-day plague.
SALT LAKE CITY —
Lynn Webster had long been fascinated by pain. As a boy growing up in Nebraska, he’d watch his grandmother spend the day looking out the window of their farmhouse, unable to move more than a few inches at a time because of advanced multiple sclerosis.
When the pain got really bad, and his grandmother would writhe or scream out, pleading to God for relief, the young Webster would press her feet to the floor until the pain passed. It was a lesson he never forgot, taking it with him to his medical residency at the University of Utah, and within years it propelled him to the top of what appeared to be a remarkable new horizon in medicine: treating pain as a disease.
“The same type of thing you would have with a music scene, where you would have a lot of people interested in the same thing, happened in Salt Lake with pain medicine,” said Sam Quinones, author of "Dreamland," a book that explores the roots of the opioid epidemic. “There was a lot of collaborating between doctors, sometimes competing. A lot of them understood that they were looking for new ways of alleviating pain. They became great proponents in the opioid scene.”
No doctor in Salt Lake City had a bigger influence than Webster. He wrote numerous studies that touted the benefits of opioids, served as president of the American Academy of Pain Medicine, and advanced the notion that addictive behaviors should be seen not as warnings, but as indications of untreated pain. He also worked as a consultant for drugmakers, conducted clinical trials and spoke at conferences around the country sponsored by Big Pharma. During what Quinones calls the “American pain revolution,” Webster became a national thought leader, and his ideas were accepted by doctors around the country.
This is the untold story of how Utah became a mecca for doctors interested in using opioids to treat chronic pain and how their well-intentioned ideas may have contributed to a national crisis. It’s also the story of a doctor at the center of the controversy, the Drug Enforcement Administration investigation that nearly derailed his career, and the hundreds of lives lost along the way.
The epidemic
Last year, roughly 64,000 people in America died from opioid or heroin overdoses, outpacing every other cause of death. This year, that number is expected to be even higher.
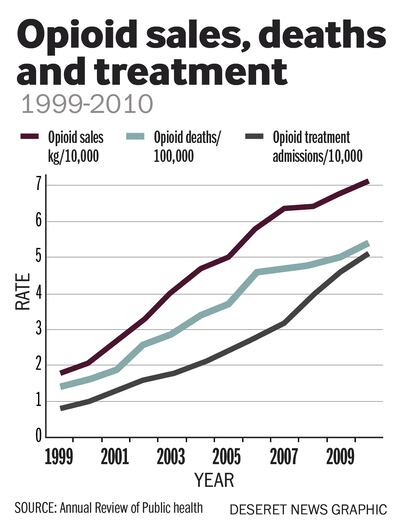
Most are dying from heroin or a synthetic analogue called fentanyl, but there’s little debate about the deeper roots of the crisis: According to a Centers for Disease Control and Prevention report in 2011, it was caused by the proliferation of painkillers and the doctors that prescribed them.
Between 1999 and 2010, pharmacy retail sales of opioid painkillers, obtained through doctor’s prescriptions, quadrupled. Deaths associated with those drugs also quadrupled.
In September, 41 attorneys general, including Utah's, issued subpoenas to major drugmakers in an effort to learn whether they intentionally misled patients and doctors about the efficacy of opioids for treating chronic pain while downplaying the risks of addiction.
Earlier this year, the attorney general of Ohio sued some of the nation's largest pharmaceutical companies for their role in helping to "unleash a health care crisis that has had far-reaching … and deadly consequences." The lawsuit alleges these companies spent millions to "falsely deny or trivialize the risks of opioids while overstating the benefits of using them for chronic pain," and it lists two doctors allegedly selected and funded by Big Pharma to support the benefits of opioids: Dr. Russell Portenoy, a prominent New York pain-care specialist; and Dr. Lynn Webster, the co-founder and chief medical director of LifeTree Clinical Research, an “otherwise unknown pain clinic in Salt Lake City, Utah.”
As the Ohio lawsuit notes, Webster was president of the American Academy of Pain Medicine and the author of numerous studies sponsored by Big Pharma. He also received significant funding from pharmaceutical companies, including nearly $2 million from Cephalon, according to the lawsuit. During the same time, he was under investigation for overprescribing by the DEA, which raided his clinic in 2010. "Although the investigation was closed without charges in 2014," the suit reads, "more than 20 of Dr. Webster's former patients at the LifeTree clinic have died of opioid overdoses."
Today, Webster says there were things doctors didn’t know about opioids and addiction, and stresses that he never advocated opioids specifically.
He says he was simply looking for more effective ways to treat pain, which remains his passion as a doctor and researcher.
“We did have some overdoses," Webster told the Deseret News. “I’m saddened I couldn’t do more for these people. That’s my only regret in my career: that I was not able to help people enough.”
Patients or victims?
The LifeTree pain clinic, which opened in 1990 and closed in 2010, served patients on referral only. Webster said most of his patients had already seen five to six doctors for chronic pain, to no avail. “They came to LifeTree because they couldn’t get relief anywhere else,” he said.
Tina Webb, who started seeing Webster in 2004, was a fairly typical patient.
Born in Bountiful, Webb was raised a member of The Church of Jesus Christ of Latter-day Saints, graduated from BYU in 1992 and married her husband, Bruce, in the Salt Lake LDS Temple. Bruce was a self-employed plumber; Tina stayed home raising their three sons.

Like many patients who ended up at LifeTree, Webb suffered chronic pain from conditions that were hard to diagnose. Looking back, Bruce thinks she might have had postpartum depression. She often complained of crippling migraine headaches and was eventually diagnosed with a disorder known as temporomandibular joint disorder, in which pain radiates from the jaw.
In 2004, an investigator with the Davis County district attorney showed up at the Webbs' house in Kaysville and informed the couple that Tina was being charged with prescription drug fraud. As part of her plea deal, she agreed to get help and was referred to LifeTree.
By 2004, Webster had seen thousands of people like Tina Webb. In his book “ The Painful Truth,” he writes that chronic pain patients like Webb are largely stigmatized. He tells the story of an incident at his clinic in 1990 that proved foundational to his practice, and his ideas about treating pain.
“I saw a patient I’ll never forget,” Webster writes. “She was a middle-aged woman with an unsmiling expression and shoulders that sagged as she sat on the end of the examining table.”
When Webster asked her how he could help, he saw “a light of hope that hadn’t been there before suddenly flickered in her eyes. I wasn’t rejecting her or putting her off.”
The patient proceeded to share with Webster a “tale that would soon grow familiar … of developing severe chronic pain, of being passed around by doctors, of being ignored or misunderstood by her so-called friends. And still the pain went on.”
When Webster opened his pain clinic in 1990, the world of medicine was in the midst of a paradigm shift on using opiates.
Two doctors in New York, Kathy Foley and Russell Portenoy, had written a widely cited paper in 1986 declaring that opiates themselves weren’t inherently addictive. That started other doctors exploring the idea that opioids might be prescribed to people suffering from chronic pain, not just those dying of cancer. At the same time, researchers were learning about how pain happened in the brain, and developing new drugs to treat it.
In 1995, the FDA approved OxyContin, a drug manufactured and distributed by Purdue Pharma, which claimed it was a medical breakthrough that allowed a controlled time-release of the narcotic, thus greatly reducing the risk of addiction.
When the Webbs came to LifeTree, Bruce said he trusted Webster could help his wife find relief from pain without addiction to opioids.

“My guard was down,” Webb recalls. “When she got in with the pain clinic I thought, ‘OK, we’re with the specialists, we have the right doctors doing the right things.’”
Within eight to nine months, Bruce said Tina started behaving strangely. She would fall asleep in the middle of dinner while eating or get up in the middle of the night and sleepwalk.
What scared Bruce the most were the times his wife would gasp for air in the middle of the night and he’d have to touch her to make sure she was still breathing.
Bruce began counting his wife’s pills to see if she was taking the prescribed amount and discovered that she was taking as many as 32 pain pills a day. Bruce said in one eight-day period, his wife took 296 pills.
After she accidentally wrecked their car into their house in June of 2006, Webb said he called LifeTree to complain about his wife’s erratic behavior, but he said that little changed in her treatment.
“When she was on the medication, that was the only thing she cared about, and the only thing she was worried about was how she was going to get more,” Bruce recalled. He wondered if his wife had become a drug addict.
He expressed his concerns to his LDS bishop.
“What are you going to do when you come home and find her dead?” Bruce recalls his bishop asking him.
Bruce said Tina agreed to get counseling through the IHC Mental Health Clinic but only went twice.
He said he then tried to convince her to enroll at private rehab centers in Florida and Arizona that charged $2,000 a day, but Tina refused. In the summer of 2007, she quit all her meds cold turkey to try to get off pain pills and went into withdrawal that induced the same symptoms experienced by heroin users — nausea, vomiting and diarrhea.
“We had a few good days and I thought, ‘Maybe this is going to be all right. But then she said she couldn’t take it anymore and she was going to go back (to LifeTree).
On Sept. 24, 2007, not long after going back to LifeTree, Tina overdosed.
When Bruce came home that night his boys, then 10 and 6, were outside playing.
“Mom’s in bed,” one of them told him. By this point, it was typical for Tina to spend most waking hours on the couch or in bed. “She won’t get up,” one of the boys said.
Bruce wasn’t alarmed; this had become routine. But when he got in the room and touched his wife, her flesh was cold. Tina had died of an overdose. Bruce would ultimately file a lawsuit against Webster.
Disturbing findings
By the early 2000s, the Utah state medical examiner, Todd Grey, had begun to notice an unsettling phenomenon in the morgue: an alarming number of drug overdose deaths tied to prescription opioids.
He alerted the state health department of his findings and an epidemiologist on loan from the CDC named Christy Porucznik looked over his data. “Our initial hypothesis was that it was possible Dr. Grey had noticed a few of these deaths and so now that’s what he’s paying attention to,” Porucznik said.
She spent months systematically sorting Grey’s data. Then she ran the numbers. She couldn’t believe what she was seeing. So she ran them again, just to be sure.
“I was shocked,” Porucznik said. In 10 years, Utah had seen a 700 percent increase in opioid-related overdoses. They were looking at an epidemic. And it would only get worse.
In 2005, Porucznik presented her findings to the CDC. The report was groundbreaking, and one of the first warning signs nationally of what would become a full-blown crisis.
At the state level, Porucznik began working with lawmakers to address the problem. First, they allowed more access to the state’s controlled substance database to get a better handle on which types of drugs were killing people most often, and where they were coming from. Were doctors overprescribing? Or were pills ending up on the street?
In 2007, Webster had issued his own guide for practitioners titled “Avoiding Opioid Abuse While Managing Pain.” The book held that opioids were still the best treatment for chronic pain and that pain was still undertreated in America.

Opioids were not “without significant risk,” he wrote, but it was important to remember that they were “used to control pain and improve function far more frequently than they serve as agents of destruction.” Those who became addicted represented a “minority,” Webster wrote. “There is no arbitrary ceiling beyond which a dose of opioids is unsafe … a physician cannot be said to be ‘overprescribing’ opioids solely on the basis of the quantity and frequency of prescribing.”
At LifeTree, Webster was guided by the idea that pain was a disease, like cancer, and that like cancer there were specific treatments for specific kinds of pain.
The prescribing patterns of his clinic reflected this philosophy. In 2007, for example, an Ogden woman named Carol Bosley came to LifeTree seeking relief for pain that radiated from her neck down to her foot. Bosley had been to LifeTree before; in fact, she’d been seeking treatment for debilitating pain for years, according to her husband.
Bosley had grown up in Ogden, and like Webb, she had married in an LDS temple. She and her husband were devout members of the LDS Church. “The church was everything to us,” her husband, Roy, recalls.
The two had met at the McKay-Dee Hospital in Ogden when Carol was studying to become a nurse and Roy was planning to go into child psychiatry. Instead, he’d become a successful construction executive and was often on the road.
In 1998, at the age of 51, Carol got into a car accident that required multiple surgeries on her neck.

“She was in constant pain,” Roy remembers. “She couldn’t sleep. The pain was so bad it would bring her to her knees. Sometimes she’d say, ‘I don’t know how much longer I can go on like this.’”
Roy noticed Carol had started doing strange things, like putting ice cream in the cupboard. Their grown children stopped visiting because Carol had a hard time carrying on a conversation. But Roy said that when he confronted his wife she became agitated and defensive.
And so Roy started taking pictures of Carol at the kitchen table, seemingly unconscious, with oatmeal dribbling out of her mouth, or passed out on the floor with a shoe held to her ear as if it were a phone, to convince her. But the pictures had little effect.
At LifeTree, she was telling the nurse practitioners who worked under Webster that she wasn’t getting much relief for her pain. A particular pill might work for a few weeks, and then its effects would wear off. Consistent with Webster’s belief that pain is a disease, and that the right type of pill can treat it, the clinic experimented with a variety of drugs and new therapies to help Carol over the years, according to documents provided by the family.
Roy noticed that Carol was hiding her meds from him, and that she was secretive and paranoid about her appointments with LifeTree, making sure Roy didn’t know when she was going in to get a refill on her prescriptions.
“I thought she was being overmedicated,” Roy said. “I didn’t have specific knowledge of the whole opioid thing. I’d heard about heroin and stuff like that, but there’s no way in the world she’d ever do something like that. She was a straight-arrow. She’d only take what her doctor prescribed.”
Roy said when he called the clinic to complain he had a hard time getting through to Webster and was frustrated that HIPPA privacy laws prevented the clinic from sharing information with him without Carol’s consent.
On May 14, 2008, Roy visited LifeTree with Carol. According to nurse’s notes summarized in documents provided by the family, Roy said his wife had a “compulsive overuse problem with drugs of all kinds,” which Carol denied. When the nurse asked Carol to produce pills that should have been left over from the previous visit, she couldn’t, leading the nurse to believe she did in fact have a “control problem … however, I believe her motivation is pain relief, not addiction.”
For the next year, Carol continued to visit LifeTree, where nurses under Webster’s direction tried a bevy of therapies, Bosley said. But in July of 2009, Carol told LifeTree her pain was getting worse, according to the summary of the nurse's notes.
On Nov. 18, 2009, her nurse wrote that he was “increasingly concerned” with Carol’s use of muscle relaxants and sleeping pills, perhaps because in the past, these had made her forgetful of how many pain pills she’d taken, resulting in overdose.
A week later, Roy came home at 3 p.m. The next day they were going to their oldest son’s house for Thanksgiving. Carol and Roy had planned to make the stuffing that afternoon, and she had asked Roy to stop by Kneader’s to get bread crumbs.
He found Carol in the den, facedown. The phone was still in her hand.
“My first thought was she was unconscious,” Roy said. But then he saw that her feet were purple. He called 911 and stared CPR. But Carol was already dead.

Last month, Roy attended the wedding of his oldest granddaughter in the Salt Lake Temple. An hour later, he sat in a restaurant across the street from Temple Square and talked about losing Carol four years ago.
“The pain is ongoing,” he said. “I’m sitting there in the temple today and I’m the only one there without a spouse.” Roy paused, his voice catching with emotion. “That young lady that was married today was very, very special to Carol Ann. She should’ve been there today.”
Roy said that it took him years before he could talk about his wife without breaking down in tears.
“It’s still hard,” he said.
The investigation
The same year Carol Bosley died, the DEA began investigating LifeTree. According to two agents who worked the case and spoke on condition of anonymity, the complaint had begun with the state medical examiner’s office, which had reported a high number of opioid related overdose deaths from patients treated at LifeTree.
By that point, the thinking on opioids had begun to shift. In 2007, Purdue Pharma and three executives had pleaded guilty in federal criminal court for misleading regulators, doctors and patients about the addictive risks of OxyContin and had agreed to pay over $600 million.
On Aug. 27, 2010, the DEA raided LifeTree. When an agent handed Webster a court order to look at medical records, Webster recognized some of the names as patients who were either using unusually high doses of opioids to deal with pain or had exhibited signs they were abusing drugs and had been discharged from LifeTree as a result, according to his book, "The Painful Truth."
An agent who worked the case said he saw an entire filing cabinet in LifeTree labeled “deceased patients.” Ultimately, the DEA seized the records of dozens of patients who had died while under the care of LifeTree, according to the agent.
Agents began meeting with surviving family members. “We’d get the same story from each of them: ‘Hey, you know, I was very concerned with the drugs and the quantities they were getting, they had overdosed a number of times, he had wrecked the car, he would fall asleep with his face in the food and aspirate and almost die,’ that sort of thing,” one of the agents on the case recalls.
The DEA spent four years investigating Webster, and while the agents thought they had plenty to build a criminal case, the U.S. attorney ultimately declined to prosecute because of a lack of evidence. One DEA agent who worked the case called it the most frustrating of his career. The U.S. Attorney's Office declined to comment.
The reckoning
The industry that flooded America with opioids is now under attack, and so are the doctors who helped them. There are lawsuits pending against pharmaceutical companies in Illinois, Mississippi, California, New York and dozens of other states and cities. It’s a strategy that echoes the effort against Big Tobacco in the 1990s, when 46 states entered into the largest civil-litigation settlement agreement in history.
Nowhere has been harder hit by the opioid crisis than Ohio. In 2012 alone there were 793 million doses of opioids prescribed in the state, enough to supply every man, woman and child with 68 pills each, according to the Atlantic.
In a lawsuit filed in May, Ohio Attorney General Mike DeWine lays at least some of the blame at the feet of doctors like Lynn Webster and Perry Fine, currently at the Pain Management Center at University of Utah Health. (Although neither Webster nor Fine are named as defendants in the lawsuit, they are mentioned as national thought leaders on treating pain with opioids.)
The Ohio lawsuit said Webster and Fine were among a group of doctors funded and directed by Big Pharma and alleges that Webster created treatment guidelines for opioids, was a "leading proponent of 'psuedoaddiction,' the notion that addictive behaviors should be seen not as warnings, but as indications of undertreated pain," and participated in “front groups” that pushed opioids.
“Whatever claims are being made are absolutely false,” Fine told the Deseret News in June, stressing that he did not downplay the risks of opioid use to patients or doctors.
In 2015, Webster received nearly $100,000 in payments from pharmaceutical and medical device companies, mostly for consulting and promotional speaking. Last year, he received $173,511 in research funding, according to Open Payments Data, a federally run transparency group that collects information on the relationships doctors and hospitals have with health care manufacturing companies. According to the database, from 2013 to 2015 Webster was listed as the principal researcher on just over $9 million worth of contracts with pharmaceutical companies, including Pfizer Inc., Mallinckrodt LLC, Bristol-Myers Squibb Co., Jazz Pharmaceuticals Inc., and Orexo US Inc.
Doctors like Webster were once considered cutting-edge practitioners in the field of pain, which for a time was seen as one of the most exciting and innovative areas of medicine, said Anna Lembke, chief of addiction medicine at Stanford University School of Medicine.
But now, the ideas Webster espoused are considered outdated, Lembke said. Today, the “standard of care” established by the CDC is that opioids are not actually effective for treating chronic pain. Lembke said anyone taking more than 90 to 120 morphine milligrams equivalent daily should either be tapered down to a safer amount or taken off completely.
Lembke said doctors like Webster were for the most part well-intentioned, operating with the current understanding they had. When she looks back on the causes of the opioid crisis she said blame does lie at the feet of doctors, but it also lies with pharmaceutical companies, the medical insurance industry, patients themselves and something she calls the "Toyatization" of medicine: an efficient, streamlined corporate process that pushed family practice doctors out and replaced them with doctors incentivized and pressured to move patients in and out as quick as possible to maximize profits and avoid complaints.
“The pharmaceutical industry used a Trojan horse approach,” Lembke said. “They convinced doctors that prescribing opioids for chronic pain was supported by evidence, when in fact there’s no evidence to support the use of opioids for chronic pain and growing evidence that it causes harm when used daily for more than three months.”

As Lembke writes in her book "Drug Dealer, MD: How Doctors Were Duped, Patients Got Hooked and Why It’s So Hard to Stop," sustained heavy use of opioids causes biochemical changes in the brain that keeps the substance from having its desired effect, creating a craving for more and more to get the initial response, an effect similar to heroin.
“We have to acknowledge that the experiment of using opioids for chronic pain is a failed one,” Lembke said. “Having said that, we now have millions of people who are the victims of the way we have practiced pain medicine for the past two decades, who have been now on high-dose opioids for a long time, taken as prescribed by a doctor. Those individuals may have to be on some level of opioids the rest of their lives because their brains have been permanently altered by exposure to those opioids. But still, even those people — it should be acknowledged that what we’re essentially treating is not the underlying pain condition, but an opioid dependence, and they should be on safe doses.”
The medical field has already begun to self-correct. In Utah, for example, a group of emergency room doctors at Intermountain Medical Center have started a voluntary initiative to limit the number of pills they prescribe.
The state has also given doctors access to the controlled substance database, which allows them to assess the prescriptions a patient has. This has helped doctors and nurses curtail the practice known as “doctor shopping,” in which patients addicted to pain pills go from one clinic to another until they can get the prescription for the pills they want.
“What happened in Utah is what’s been happening across the entire country,” said Dan Ciccarone, a professor of family and community medicine at the University of California, San Francisco, and an expert in heroin use. “There was a generational change in attitudes of how to treat pain. It wasn’t just the doctors; it was a cultural shift.”
And yet, Ciccarone and others point out, if the pendulum swings too far in cracking down on opioid use, patients who really need them could be hurt.
“We created the medicine for a reason. It’s incredibly useful,” Ciccarone said. “If you’re anti, meaning trying to put the genie back in the bottle, that’s unreasonable. That’s like saying we want the combustion engine to go away because it’s causing too much pollution. … We need to learn to use opioids better, we need to be more responsible. We need to create a modern stance between the two poles.”
Moving forward
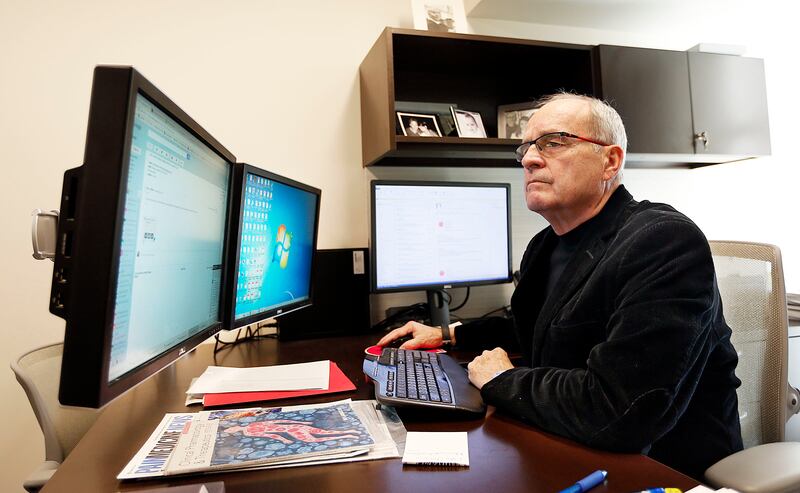
It’s a warm afternoon in September, and Lynn Webster is at his office at PRA Health Sciences. He rarely prescribes pain medicine these days, other than as part of clinical trials. Today, his main focus is on research.
Seated in his office, which has virtually no personal effects, Webster makes no apologies for his close ties to Big Pharma; it’s how research gets done, he said. When a pharmaceutical company hires his firm to do clinical trials, 90 percent goes toward the cost of the trial — blood work, expensive new equipment, lab time and salaried nurses. Without pharmaceutical companies bankrolling these studies to find safer and more effective drugs, “there would be no research,” Webster said. “There would be no advances.” (Lembke said this isn’t true. “That’s what the NIH [National Institutes of Health] is for,” she said).

Webster said he’s often misunderstood. He points out that he was one of the first people nationally to speak out about the dangers of opioids and overdoses. In 2006, he started a foundation called LifeSource that was dedicated to stopping opioid deaths (the foundation closed in 2010).
“Almost all of what you hear about today is about the harm of opioids. And there is a lot of harm. It’s tremendous, it’s terrible,” Webster said. “But in that narrative the people in pain are being forgotten.”
Webster said that almost weekly he gets emails or phone calls from people who are suicidal because doctors will not prescribe them opioids.
As for the families of people like Bosley and Webb — and others who were part of a now-settled lawsuit against him — he chooses his words carefully.
“I refuse to talk about any of my former patients ... there are some things I can’t legally say because of HIPPA (privacy laws) that are in the chart that they all know because it was in the chart,” Webster said. “But more importantly than that is I can’t, and I won’t, I wouldn’t criticize a family of somebody who died. I cannot do that because that’s just not right. I’m not going to do that.”
From time to time, Webster still thinks back to his grandmother in Nebraska all those years ago, and the way he did his best to ease her pain. As he writes in "The Painful Truth," he was never able to treat her pain from multiple sclerosis; she died in 1970 while he was still in college. But looking back, he writes that he wonders if he was more help than he realized at the time.
“With me by her side, she knew she wasn’t alone in her suffering,” Webster writes. “She had someone who would keep her company and talk with her, someone who loved her … what if a little help from others was all it would take to feel better?”
Treating people with chronic pain is the basis of Webster’s motivation, he said. It’s why he prescribed opioids to treat chronic pain, why he conducts clinical trials and why he even wrote a book to defend and explain himself. He said he never advocated for opioids specifically and clarifies that his main goal was simply to help people in pain.
When he thinks back on the patients he’s helped over the years, he feels a deep sense of satisfaction. But ask him about the ones he lost, and the ones who sued him and blame him for killing their loved ones, and his face clouds with the very thing he’s spent his life trying to eradicate: pain.
“I know that the conduct of the care, the care that was provided had all the right intentions and we did as well as I think anybody could have done — but it wasn’t enough.”
Webster looks at the time and politely excuses himself. He must go to another wing of the building.
He has research to conduct.