





Three years ago, researchers from Utah State University and the University of Utah convened with the Great Salt Lake Strike Team alongside state agencies to sound the alarm. A team of scientists led by BYU soon followed with a warning that the Great Salt Lake could essentially disappear within five years — a collapse that would pollute the air for millions and cripple the regional economy — unless Utahns cut their water use by a third or more.
Multiple forces united. State monies were allocated, along with a proposed $1 billion from the White House. A coalition of business and nonprofit leaders — led by Josh Romney’s Great Salt Lake Rising and including the conservationist group Ducks Unlimited — pledged hundreds of millions more. Those involved were aware that when a life-giving resource is at risk, it is essential to channel every potential source.
American health professionals and the general public could stand to learn from that resolve to preserve and leverage a precious asset. Because faith and religious community — resources strongly tied to a longer and healthier life — are ones our health system rarely acknowledges.
How religion impacts longevity
The United States spends more per person on healthcare than any other wealthy nation, yet Americans live shorter lives than people in nearly all of them. A 2025 Lancet analysis also found the U.S. has made unusually poor progress against chronic disease, with mortality rising among adults aged 20 to 45 — the same generations who are now least connected to religious community. Pew also reports the share of religiously unaffiliated adults has nearly doubled since 2007, to roughly 29% today. The combination of this data should make us curious.
Look closely at the Intermountain West and the curiosity sharpens. Utah posts the lowest adult smoking rate in America — just over 7% — alongside one of the lowest rates of physical inactivity. Researchers have long attributed much of that advantage to the region’s dominant faith — The Church of Jesus Christ of Latter-day Saints — and its health code, which forbids tobacco and alcohol use while extolling activity and family.
The numbers behind this link are striking. A landmark UCLA study followed nearly 10,000 devout California Latter-day Saints and found that active Latter-day Saint men were living 8 to 11 years longer than the U.S. average.
The pattern is not unique to one faith. In Loma Linda, California — the only “Blue Zone” of exceptional longevity in the United States — Seventh-day Adventists outlive their countrymen by close to a decade, with markedly lower rates of heart disease and cancer. Further research found the faithful, across denominations and faiths, who attended weekly or more live 7.6 years longer — 13.7 years longer among African Americans.
Religious involvement as health enhancer
Imagine a low-cost therapy with years of life-boosting influence going unmentioned by a medical expert.
This fall, the Centers for Medicare and Medicaid Services will launch MAHA ELEVATE, a roughly $100 million model testing “whole-person care” for Medicare patients. Its priorities — nutrition, physical activity, sleep, stress management, social connection and avoiding harmful substances — are all worthwhile. They are also notable for what they omit: the factor of faith community involvement.
In a new report from the Wheatley Institute, we analyzed findings drawn from Oxford University’s three Handbooks of Religion and Health, covering the best existing research in the field. Of 1,069 high-quality studies across 15 physical health domains, 876 found positive associations between religious involvement and physical health and only 124 found negative ones — a ratio of roughly 7 to 1.
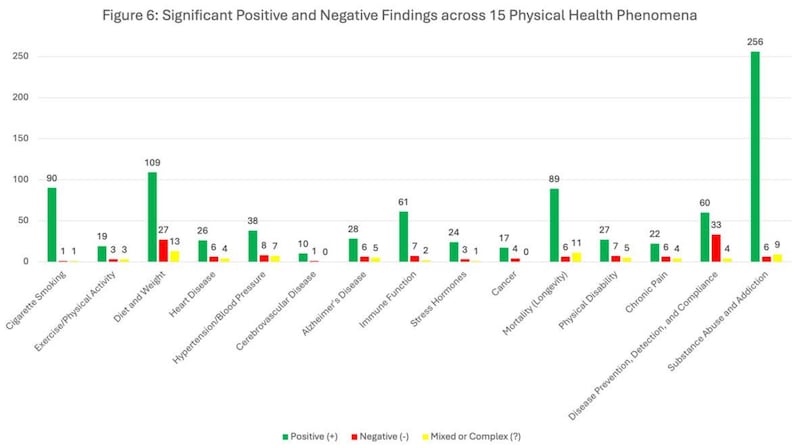
The strongest signals come from the same areas that American medicine spends the most time and money on. Among high-quality studies of cigarette smoking, “significantly” positive findings outnumber negative ones by 90 to 1; on substance abuse and addiction, 43 to 1; on mortality and longevity, 15 to 1.
How faith impacts the body
Religious communities shape behavior and accountability. They discourage the habits that fill cardiology wards — smoking, heavy drinking, sedentary living, social isolation — and reinforce habits that keep hearts and bodies healthy. They build networks of care that last decades, not just the length of an annual physical. And these same faith communities give people reasons to get up, get out, serve and look after a neighbor.
Here is an irony: Utah is among the most religious states in the union and one of the healthiest. Yet even here, the medical system rarely treats a patient’s faith community as the health asset it is. The new federal prevention model leaves it off the list. We fight over every acre-foot of water and still let this other wellspring run unused.
In Memphis, Methodist Le Bonheur Healthcare formalized covenant agreements with roughly 500 congregations, embedding trained liaisons in each to follow patients from admission through recovery. The results: mortality was less than half the comparison rate, and enrolled members had meaningfully lower healthcare costs — a model the Journal of the American Medical Association cited as a best practice and that Wake Forest’s FaithHealth program later replicated in North Carolina. The evidence is strong enough that Health Affairs, the nation’s flagship health policy journal, devoted a 2024 issue to reimagining public health — featuring a call by Harvard public health researchers for spirituality to be formally recognized as a social determinant of health, with the same policy infrastructure we give diet and exercise.
The researchers were clear that the evidence base is physical as much as spiritual: lower all-cause mortality, reduced chronic disease, longer life. But still, some wonder: How can we act on this?
A realistic pathway to strengthen public health
A wise approach would be voluntary, evidence-based and pluralistic. No physician can prescribe belief, but belief is not what the best research is measuring. The best studies track attendance, community membership, and shared practice — things people can choose.
The clinical conversation can sound like this: “Do you have a community outside work and family that you gather with regularly? Research suggests that kind of connection has real, positive effects on physical health. Is that something you’d want help finding?”
For patients who already belong to a faith community, the follow-up is even simpler: “Are you actively involved in it?”
We do not ask people whether they believe exercise is meaningful before recommending it. We tell them it helps and let them decide.
Intermountain Health, headquartered in Salt Lake City and serving six states, already has a community health arm and an explicit faith ministry presence after its 2022 merger with SCL Health. As a Catholic system founded by the Sisters of Charity of Leavenworth, it carries an explicit faith ministry presence in its own hospitals.
Utah’s dense congregational networks — where members are already assigned to watch over and minister to one another in love — are the informal version of what Memphis had to build from scratch.
A system serious about adding years to American lives should stop overlooking one of the most durable, low-cost sources of discipline, belonging and longevity.
No single intervention will fix American health. But a system serious about adding years to American lives should stop overlooking one of the most durable, low-cost sources of discipline, belonging and longevity. Doctors need not proselytize, and government need not favor any creed.
In the West, we are mobilizing billions and uniting old rivals to rescue a dying lake. We should be at least as willing to tap a wellspring of health that is already all around us.